

When I think about growing up in the late 1970’s, I have strong memories of dealing with an energy crisis. President Carter and my dad both installed solar panels on their houses. Almost every building, store and school took out half of the light bulbs. And we all wore sweaters in the winter: ugly shapeless sweaters. Today we face an environmental crisis of greater magnitude; as an architect, I realized that I have an opportunity and the responsibility to influence a much more effective response.
A few years ago, I started looking much more closely into how much energy the types of projects that I work on consume: it’s a lot. It turns out that Healthcare is the second most energy intensive building type in the country, accounting for almost 10% of all building energy use according the US Energy Information Administration. Looking out even further, that’s about 5% of all energy consumed in the United States today including energy for industry, transportation, and building infrastructure. Can I do anything to help ease this massive burden? Yes, I believe that I can.
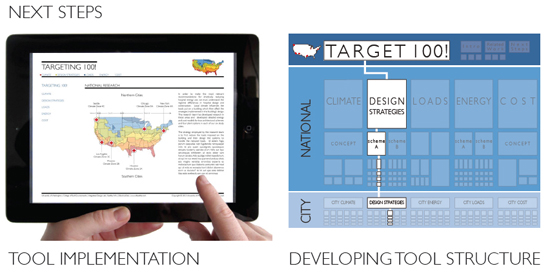
About two years ago during project research, I came across the “Targeting 100!” report by the University of Washington [UW] Integrated Design Lab about reducing energy use in hospitals. I knew that I had to share it. In October the BSA and a diverse group of industry sponsors helped bring the UW researchers, Heather Burpee and Joel Loveland, to Boston. In presenting their work, they ignited a series of discussions on how we can make a difference to reduce energy consumption.
Begun almost five years ago as an interdisciplinary effort, their research looked at how a number of overlapping techniques could contribute to lower energy use and achieve a target: 100 kBtu per square foot per year. This goal is a 60% energy use reduction from the current US average and it would fulfill the 2030 Challenge. Adopted by the AIA, PAYETTE (where I work) and many other firms and organizations, the goal of the challenge is to reduce energy consumption incrementally over twenty years to net zero.
Why start at targeting 100? Putting it in perspective, the average US hospital today uses between 250-350 kBtu/sf per year; the average office building is between 80-100 kBtu/sf per year. However, the researcher found that the average hospital in Northern Europe uses around 100 kBtu/sf. Why is this? It comes from many factors including alternate code focuses, higher energy costs, and different cultural values.
In the presentation and reports, the message of Targeting 100 is one we know well: building should heal and not hurt. However, it is the simultaneous depth and breadth of the research that elegantly codifies this.
No single system or solution will achieve everything, but many overlapping methods can. First, build a well-insulated envelope. Second, protect glazing from solar radiation to reduce peak system loads. Third, separate the ventilation systems from heating and cooling systems and utilize displacement air delivery. Fourth, implement high efficiency boilers and chillers (with geo-thermal or co-generation as good alternates.) Unfortunately, we all know that getting things like these into our projects is easier said than done.
Where the Targeting 100! research excels is in testing first- and life-cycle costs benefits to make these system integrations feasible. Last year a US Department of Energy grant expanded the initial work in the Pacific Northwest to the nation’s other most populous climate zones, with the ultimate goal of an on-line tool to help us (architects, owners and engineers) educate others and implement their findings. There are some difficulties, though. The research focuses primarily on solutions for new construction and, regardless of the project type, separation of construction and operations budgets protect the status quo of practice.
I am encouraged that Targeting 100’s message is becoming more familiar across the US. In New England, a greater opportunity awaits. We don’t build many new hospitals here, but we do have some of the oldest and most valuable building stock in the country. I believe that we can bring together professional practice, academia and the construction industry to tackle the pressing issue of renovating for healthcare. Extrapolating this research into a practical set of guidelines for healthcare in the Northeast and beyond is smart and reasonable. It’s healthy for people, our profession, our economy and our environment.
Related Links:
Targeting 100!
It’s not an Engineering Problem
Cover image: UW-IDL
{kind=link}
Sandrine Héroux, Sophie McKenzie, and Emily Chowdhury are each members of our in-house Fabrication team. Their day-to-day work centers on a simple question: what changes when design becomes something people can physically test?
These women challenge the notion of fabrication as a support service, framing it instead as an essential component of architectural authorship, a way to test ideas, share agency, and widen the boundaries of what architectural practice can include.
In our most recent blog, they discuss their individual paths in architecture and reflect on their experience using fabrication as a tool for fostering shared agency, community engagement and broadening the role of the architect. Link in bio!
#designalways #artofmaking #architecture #madamearchitect #womeninfabrication #fabrication #bostonarchitecture #bostonfabrication #archdaily #archisource